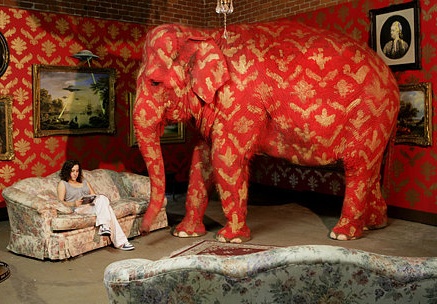
There are (at least) three big elephants in the room when it comes to senior housing. One has received some attention in the press and the other two seem to get no attention in the industry press:
- Sexual relationships between Seniors – There have been some court cases and some articles about sexual relationships between residents. While I have not published anything on the topic, I have seen a few articles written about it. The issue has received some attention because of abuses or alleged abuses and it is a difficult issue because there are so many seniors who have some degree of diminished capacity.
Within this realm I have not seen anything written about sexually transmitted diseases. I know that in younger, more active senior communities it has become a significant issue but maybe that is not true assisted living communities.
- Elopement – More than a year ago, I attended a breakout session on elopement at the Oregon Healthcare Association Annual meeting. I was particularly interested because of my relationship with Vigil Health Solutions and our call system designed specifically for residents with dementia who cannot use a traditional call system.
I expected the crowd to be small but it was packed, leading me to believe that elopement is a big issue for many/most senior communities. But, I believe, there is a real reluctance to talk about it because of the possible legal jeopardy.
- Excessive Drinking – There is no question that a significant percentage of the senior population drinks too much. For the most part they are silent and mostly invisible drinkers, which makes the problem easier to overlook or to treat as a resident’s personal business. That being said, caregivers know: they see the empty containers, the physical symptoms. The question is really this, if residents quietly drink to oblivion every night in their own room and they are not causing disruptions, is that okay or do we as senior care providers have an obligation to get involved?
This is mostly an article to raise some questions:
- Do I have it right that these are elephants in the room?
- Are there other secret or silent issues we should be talking about?
- If you have stories or thoughts on the silent problems I would love to have you share them as a way to address the issues with more depth either in the comments below or in a private email.
Steve Moran
If you like this article (or even if you don’t) it would be a great honor to have you subscribe to our mailing list HERE.



The biggest thing I hear from I hear from people and would tend to agree is most communities over promise, oversell and under deliver on care. They are just warehouses for bodies and receive 3 squares a day basically.
Unfortunately this is an industry that has high turnover issues and typically low pay for caregiver staff. This is true even in mid to high end communities unfortunately. It starts with management, and with a top hands on manager, there is a much greater chance for better care and a well run facility.
Being at the tail end of the baby boomer generation, this is not my idea of the life I want for my final years. I hope there are positive changes ahead and better pay for the people that help our seniors in their everyday lives.
Hi Steve. Even back in ’94 when I got my Post Masters Certificate in Gerontogy, we were discussing theses same issues…except for elopement, which is news to me. So the real question for us is why the elephant hasn’t been disrobed long before now? And more so, what to do about it! Your post is a starting point. Thanks. Also, let’s not forget to include the probable use of pot as the Boomer Generation moves into theses new realms.
I believe you hit the “elephant in the room” on the head. One other item I have found in my 25 years of Administrative experience is a form of spousal “abuse”. (I use this word for the lack of a more proper term…please continue to read) This is rarely talked about and is a delicate issue. I ran across this when transitioning from SNF to Retirement Community operation. There is an increasing number of couples living in IL & ALF’s and often one individual is the “lead” as in most relationships. The rub is when the lead turns into caregiving which comes with frustrations and tiresome efforts to keep things together. Most often this is done behind closed doors and generally the staff/caregivers are not being called upon due to the residents stand for control. Now- I must be clear that “abuse” does not mean “to raise a hand against the other” but to not assist with meds properly, not hydrating due to increase of incontinence, forced mobility without proper DME, decrease in medical attention and simple lack of kind words or patience with the spouse who is has a form of dementia. The list could go on & on. Do we call this “abuse”? Clearly there is not a deliberate action to harm but in some cases intervention is our responsibility. Eyes should be wide open and gentle conversations begin……….
These are real issues/elephants that are daily issues inAssisted Living and other senior care housing.
The solution is in training staff to really understand how to identify triggers or precursor behaviors so that interventions can be made before the elephants stampede!
There is one more that is coming soon, I think. As more and more baby-boomers reach the age that they will require some kind of assistance, there will be same-sex couples coming in. The biggest problem with this is the caregivers. I have had one caregiver tell me point blank that if we had a gay couple come in, she would not take care of them because she would not want to catch something. (Of course, that same caregiver wouldn’t take care of a lady who had a “personal massager,” because she thought it wasn’t right for old people to “do that.”)
Hi Steve,
I absolutely agree that these are three common ‘elephants in the room’ in long term care. I’m looking forward to future articles sharing thoughts/proposed solutions/ideas on these elephants, now that we’ve named them 🙂
From LinkedIn Groups
Employee turnover
By Anthony Esposito
From LinkedIn Groups
Hi Steve, each of the topics that are mentioned in your article are no doubt very important and as said above huge discussion points. Another subject that should get more focus but does not is quality bowel care protocol. Roughly 75% of seniors over the age of 75 tend to have constipation as a result of decreased exercise and mobility, fluid and fiber intake and most importantly medication they are taking. For decades they have been prescribed oral medications, which take a lot of time, have no predictability and at times can cause cramping, bisacodyl suppositories, which have been evidenced to injure the mucosal lining as early as 30 minutes after insertion to several hours later and cause incontinence as the suppository melts since it is not always passed at first evacuation.. Even at times of greater cases of constipation they have been given full volume enemas. A full volume enema is great as a prep for a procedure, not as a quality bowel care protocol. There are 5cc mini enemas that can provide predictability, fast and effective evacuation with no mucosal discharge, less nursing intervention and the patient is comfortable, their day doesn’t have to include embarrassment or even worse be subject to the possibility of a pressure ulcer due to skin integrity breakdown.
By Marc Weiss
From LinkedIn Groups
Steve…you have hit on most all of the “tender” issues. The other one I can think of is anorexia, which is common in many older adults. This is a method, albeit a horrible one, to control your life when you feel it is not in your hands anymore. Thanks for the read…
By Cindy Janssen
Hi Steve, I think there is another elephant in the room and that is chronic, and often undiagnosed and untreated mental illness such as bi-polar, severe depression and other diagnoses. Often families are not aware or hide the fact from communities. Being in independent living I must follow fair housing but with the right open ended questions you can find out much about the potential resident and at least be prepared when they move in. I think that many problems that have been reported in assisted living are because families are educated or even know what questions to ask and marketing staff on under pressure to fill the units. We are doing a disservice to our communties, potential residents and their families if we don’t do our best to make sure we are the right place for the particular situation.